¶ Chapter 6 — ARTICULATORS AND ARTICULATOR SIMULATION OF HUMAN ANATOMICAL CHARACTERISTICS
Reference Edition
This chapter is part of the Air Force Dental Laboratory Manual (2005) – Digitally Restored Edition.
This edition preserves the original publication while correcting OCR errors, restoring formatting, reconstructing damaged tables where necessary, and improving digital readability.
The technical content has not been rewritten, modernized, expanded, or altered.
It is provided as a professional reference. Modern instructional material is published separately throughout DentalTechnology.org.
¶ Section 6A — Types of Articulators
¶ 6.1. Overview
An articulator is a mechanical instrument that represents the temporomandibular joint and jaws, to which the maxillary and mandibular cast may be attached to simulate all or some of the mandibular movements. Articulators simulate the positions and movements of the patient’s lower jaw in relation to the upper jaw so a prosthesis with proper occlusion can be made. The accuracy of the simulation depends on the accuracy of the dentist’s transfer records and the degree of adjustability of the instrument.
¶ 6.2. Transfer Records
The following records, detailed in Section 6B are important to the process:
6.2.1. The vertical and horizontal orientation of the upper jaw to both temporomandibular joints.
6.2.2. The patient’s actual centric relation, or the dentist’s estimate of where centric relation should occur.
6.2.3. The angles that the articulator eminences form with the occlusal plane.
6.2.4. The temporomandibular joint characteristics governing the timing and direction of laterotrusion.
6.2.5. The distance between the patient’s condyles (intercondylar distance).
6.2.6. Relative presence or absence of anterior guidance.
¶ 6.3. Articulator Categories
6.3.1. There are many different kinds of articulators. The primary difference among them is in the number of controls or adjustments they possess.
6.3.2. Articulators having a full range of adjustments can be set to match the patient’s guiding anatomical features. As a result, articulator movements come very close to duplicating the patient’s actual jaw movements. Articulators with no adjustments are built to move in a statistically average manner, cannot be set to move in any other way, and have a much more limited application.
6.3.3. Based on the adjustability factor, articulators fall into three broad categories; nonadjustable (paragraph 6.4), semiadjustable (paragraph 6.5), and fully adjustable (paragraph 6.6).
6.3.4. Just because an articulator has minimal adjustability does not mean it is inferior. An articulator only becomes inferior when it is taxed beyond its capabilities. On the other hand, a fancy, impressive articulator is still only a machine unless used to its fullest advantage. The dental laboratory technician should become intimately familiar with how all types of articulators work in order to develop the ability to match a job’s demands to an articulator’s capabilities. Once an articulator is selected, the technician should not use the device beyond its mechanical limitations.
¶ 6.4. Nonadjustable Articulators
6.4.1. Hinge-Type Articulator. This variety is the simplest made. It can make a basic opening and closing movement (Figure 6.1). It has no ability to go into lateral or protrusive excursions.
6.4.1.1. Sometimes these devices are called “holding” instruments. Their only function is to hold or maintain the vertical and horizontal relationships between two casts at one mandibular position.
Figure 6.1. Hinge-Type Articulator.

6.4.1.2. Most of the time, hinge instruments are used to make very simple fixed and removable prostheses. The dentist fully expects to correct lateral and protrusive interferences in the mouth at the time the prosthesis is inserted. Examples of these replacements would be a temporary fixed partial denture or an interim RPD.
6.4.1.3. It is possible to make very complicated, “permanent” restorations with a pure hinge instrument. For a hinge instrument to be used this way, the dentist would have to use functionally generated path techniques to get adequate cast mountings for the job.
6.4.2. Fixed-Guide Articulator.
6.4.2.1. Fixed-guide articulators are machined to produce the lateral and protrusive movements characteristic of a statistically average patient (Figure 6.2). Therefore, if the “average” movements of the articulator match the actual movements of the patient, the patient is in luck.
6.4.2.2. These kinds of articulators are used extensively, and the success rate associated with their use appears to be acceptable. The ability of these articulators to hold vertical and horizontal relationships between opposing casts is their most dependable performance feature. Lateral and protrusive movement paths are only moderately dependable.
6.4.2.3. Functionally generated chewing surface techniques aside, fixed guide articulators should be used for cases where precise duplication of lateral movements is not critical. Examples of these cases are complete crowns for incisor teeth; short span anterior fixed partial dentures; posterior onlays, crowns, and short span fixed partial dentures where anterior guidance is immediate and steep; monoplane complete dentures using 0-degree teeth; and RPD construction for patients with a definite anterior-guided occlusion.
Figure 6.2. Fixed-Guide Articulator.

¶ 6.5. Semiadjustable Articulator
6.5.1. The semiadjustable articulator has enough adjustable features to give fair to good simulation of a patient’s actual mandibular movements.
6.5.2. Many articulators in this class can compensate for the angle of a person’s articular eminence, horizontal and vertical overlap conditions, and amount of progressive mandibular translation (sideshift). Some have fewer adjustments (no variable progressive sideshift), and some have more adjustments (immediate sideshift, progressive sideshift, and variable intercondylar distance).
6.5.3. These articulators are very versatile and the most frequently used in the Dental Services. They are used for making all forms of removable prostheses and for moderately complicated fixed prosthodontic restorations. Some dentists use the most adjustable of the articulators in this group for complete mouth fixed prosthodontic rehabilitations.
6.5.4. The types of semiadjustable articulators commonly used are the Hanau H2-158 (Figure 6.3), Hanau Wide-Vue (Figure 6.4) and the Whip-Mix (Figure 6.5).
6.5.5. There are two ways (methods) of using semiadjustable articulators from the standpoint of making them match the patient’s anatomical features and resultant mandibular movement.
6.5.5.1. Arbitrary (or Average) Method. Only those patient factors that are most critical to the success of the case are reproduced on the articulator with the greatest accuracy possible (for example, centric relation, MI, and occlusal vertical dimension). Statistical averages are used to set all remaining articulator adjustments. The so-called “average” settings are supposed to hold true for the majority of the patient population. When a semiadjustable articulator is used in this way, it becomes a fixed guide instrument and has the same limitations.
6.5.5.2. Semiadjustable Method. The dentist articulates the patient’s casts and sets all articulator adjustments based on actual patient measurements. Two kinds of measurement systems are used; facebow transfer and maxillomandibular relationship records, as follows:
Figure 6.3. Hanau H2-158 Semiadjustable Articulator.

Figure 6.4. Hanau Wide-Vue Semiadjustable Articulator.

6.5.5.2.1. Facebow Transfer. A facebow transfer is a procedure used to attach a maxillary cast onto an articulator in the same way the maxilla relates to the temporomandibular joints. When the infraorbital canal is used as a third point of reference in a facebow transfer, the maxillary cast is also related to the horizontal plane of the articulator like the patient’s maxilla relates to the axis-orbital plane. This transfer, in combination with a maxillomandibular relationship record, allows the opening axis of the patient to be transferred to the articulator.
6.5.5.2.2. Maxillomandibular Relationship Records. The articulator’s adjustments are set according to three-dimensional methods of measurement called maxillomandibular relationship records. There are two types of maxillomandibular relationship records. The first is a template that relates the lower cast against the upper cast in the same way the jaws relate when the record is made in the patient’s mouth (for example, centric relation record).
After the casts are mounted, the second kind of maxillomandibular relationship record is used to set articulator adjustments (lateral and protrusive records).
Figure 6.5. Whip-Mix Semiadjustable Articulator.

¶ 6.6. Fully Adjustable Articulator
6.6.1. This category differs from the semiadjustable one because of features like custom-made condyle guides, highly variable intercondylar distance, very close simulation of the timing and direction of laterotrusion, and a capacity to simulate the direction of the rotating condyle (Figures 6.6 and 6.7).
6.6.2. The information needed to accomplish these highly refined adjustments does not come from maxillomandibular relationship records. It comes from mandibular movement tracings or recordings (pantographic tracings or stereographic recordings ) made by the patient under the direction of the dentist. The articulator is then programmed to conform to the tracings or recordings.
6.6.3. Fully adjustable articulators are used on the most demanding kinds of cases; that is, detecting and treating patients whose jaw movement patterns are not normal and completing full mouth fixed prosthodontic restorations. NOTE: A fully adjustable instrument can be used in the fixed-guide and semiadjustable modes if a less adjustable articulator is not available.
¶ 6.7. Arcon Versus Non-Arcon
6.7.1. Some semiadjustable articulators and all fully adjustable articulators are described as being arcon in design. The word arcon is an acronym for the words ARticulator and CONdyle. It describes those instruments having the condyle elements attached to the articulator’s lower member in the same way condyles are an anatomic feature of the mandible in a human skull.
6.7.2. At the same time, the upper member of the articulator carries mechanisms simulating the glenoid fossae of the maxilla. As examples, the Hanau H2-158, Hanau Wide-Vue, and Whip-Mix are semiadjustable articulators of the arcon variety. The Hanau 96H2 semiadjustable articulator is non-arcon in design. Stuart®, Denar®, and TMJ instruments are fully adjustable articulators and, as such, are also arcon in design.
Figure 6.6. Fully Adjustable Articulator (With Pantographic Tracing).

Figure 6.7. Fully Adjustable Articulator (With Stereographic Recording).

6.7.3. What are the advantages of an arcon articulator over non-arcon varieties? One advantage of the arcon articulator is that it is anatomically correct, making it easier to understand mandibular movements. Another advantage of the arcon design is that the condylar inclination is at a fixed angle relative to the occlusal plane. When the arcon designed articulator is opened, the angle between the condylar inclination and the occlusal plane remains constant.
6.7.4. Perfect reproduction of mandibular movement has always been an elusive goal. Once programmed, the arcon articulator is capable of mandibular movements that are closer to the patient’s own movements. This small advantage is so important that most articulators are designed as arcon articulators.
¶ 6.8. Limitations Based on Design
6.8.1. Nonadjustable Articulators. Nonadjustable articulators, like the ones in Figures 6.1 and 6.2, are small instruments that cannot effectively reproduce mandibular movements due to the following design limitations:
6.8.1.1. The distance from the teeth to the center of rotation (axis), which passes through the condyles location, is considerably shorter than in the skull. Consequently, the patient’s hinge axis is different than the articulators, causing a change in the arc of closure.
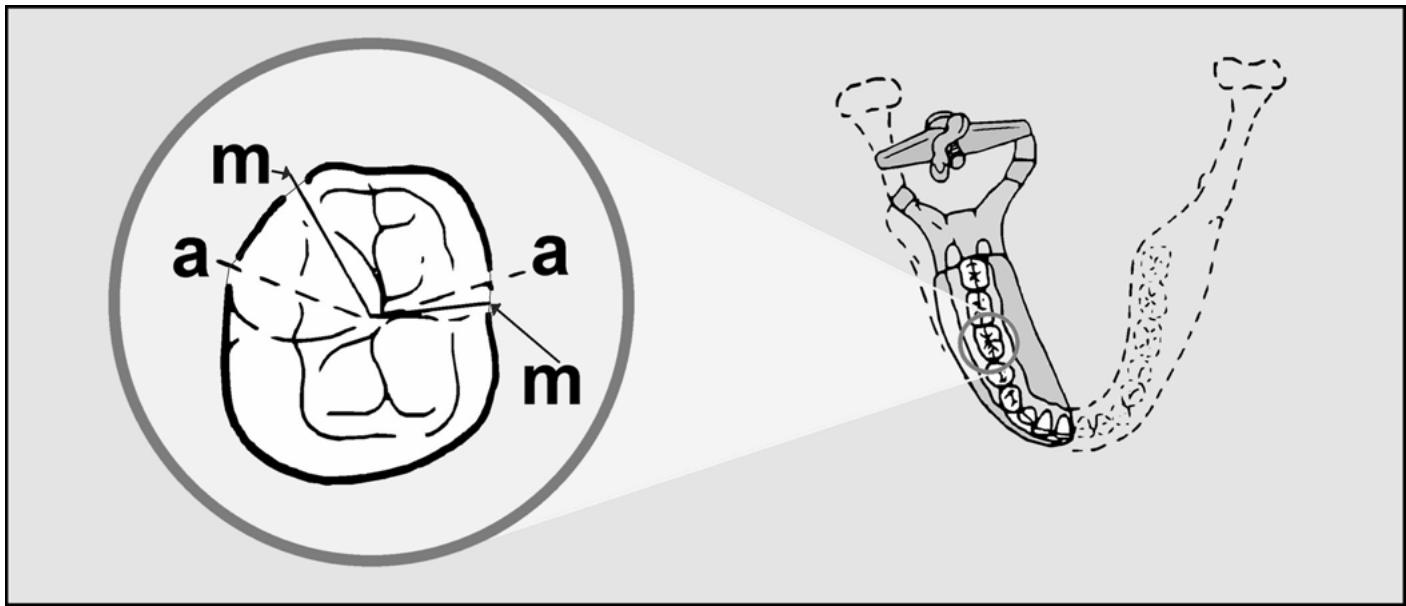
6.8.1.2. As the mandible moves up and down in the terminal hinge position, the cusp tip moves along an arc with the center of rotation located at the transverse horizontal axis shown in Figure 6.8 as the mandibular hinge axis (mha). If the distance between the transverse horizontal axis and the cusp tip differs from the patient to the articulator, the arc of closure would be different (steeper or shallower), producing an error.
Figure 6.8. Mandibular Hinge Axis (mha) Versus Articulator Hinge Axis (aha).

6.8.1.3. Drastic differences between the arc of closure on the articulator and the patient’s mouth may affect the placement of cusps, ridges, and grooves on the occlusal surfaces. For example, when casts are related using a thick interocclusal record, the teeth occlude in a different intercuspal position on the articulator than in the patient’s mouth. This results in an occlusal interference between the mesial inclines of the maxillary teeth and the distal inclines of the mandibular teeth.
6.8.1.4. If the casts are mounted in MI, without an interocclusal record, the arc of closure difference does not present a problem. The significance of “an arc of closure” depends on whether the occlusal vertical dimension is being altered. Remember, nonadjustable articulators are designed to hold and reproduce accurately only one position. If any changes in occlusal vertical dimension are foreseen, it is best to graduate to a semiadjustable articulator with appropriate facebow transfer and maxillomandibular relationship records.
6.8.1.5. The articulator’s design also effects the pathways of teeth as they travel in lateral excursions. As the distance between the condyles increases (intercondylar width), the Gothic arch angle decreases (and vice versa). This effect is even more evident when a small hinge-type articulator is used (Figure 6.9). On such small instruments, the discrepancy between the paths
traveled by a cusp on the instrument and in the mouth can be sizable, particularly on the balancing side. The result is an increased possibility of incorporating a balancing occlusal interference. NOTE: There are nonadjustable articulators approximately the same size as semiadjustable articulators. Do not assume every “nonadjustable” instrument has the same design limitations as the ones previously mentioned.
Figure 6.9. Articulator Versus Mandible Gothic Arch Tracings.
6.8.2. Semiadjustable Articulator. A semiadjustable articulator is an instrument of larger size and more closely approximates the distance from the axis of rotation to the teeth. When casts are articulated using a facebow transfer, the arc of closure produced on the articulator resembles the arc in the patient’s mouth and any resulting error is slight (Figure 6.10). Placing the casts closer to or farther away from the condyles has only a small effect during lateral excursions (Figure 6.11).
Figure 6.10. Effect of Hinge Axis Location on a Semiadjustable Articulator.

¶ 6.9. Hanau H2-158 Articulator
The parts of this articulator are listed below (and in Figure 6.12):
6.9.1. Upper Member (A)
The upper member is the articulator equivalent of the upper jaw.
6.9.2. Lower Member (B)
The lower member is the articulator equivalent of the lower jaw.
Figure 6.11. Effect of Hinge Axis Location on a Gothic Arch.


6.9.3. Mounting Plate and Lockscrew (C and D)
Mounting plates are used for fixation of the patient’s cast to the upper and lower members of the articulator. Mounting plates are keyed. The cast and its mounting plate can be removed from the articulator during work and can be replaced in the identical position.
6.9.4. Condylar Shaft (E)
The condylar shaft is the articulator equivalent of the opening and closing axis of rotation existing between the two condyles of the mandible.
6.9.5. Post (F)
The post is the articulator equivalent of a ramus of the mandible.
6.9.6. Horizontal Condylar Guidance and Lockscrew (G and H)
The condylar guidance contains a condylar slot that is the articulator equivalent of the glenoid fossa and articular eminence. By rotating the guidance, the condylar slot can be oriented at different angles. The lockscrew holds the slot at a chosen angle.
6.9.7. Horizontal Condylar Indication (I)
The horizontal condylar inclination contains a scale (-20 degrees to +60 degrees) showing the angle at which the condylar slot is inclined to the horizontal plane.
6.9.8. Condylar Element (J)
The condylar element, the ball that travels within the condylar slot, is the articulator equivalent of the condyle of the mandible.
6.9.9. Centric Stop (K)
The centric stop, a seat for the condylar element, is found in the posterior part of the condylar slot. After the maxillary and mandibular casts are mounted, the centric stop represents the position the condyle occupied within the temporomandibular joint when the maxillomandibular relationship record was made.
6.9.10. Centric Lock (L)
The centric lock is used to lock the condylar element against the centric stop.
6.9.11. Lateral Condylar Guidance and Scale (M)
Lateral condylar guidance is a progressive sideshift control. The lateral condylar guidance mechanism on the Hanau H2-158 articulator rotates laterally in and out. It rotates relative to a lateral condylar guidance scale found on the top of the upper member. The scale reads between 0 and 30 degrees. When the lateral condylar indication is higher, the progressive sideshift is greater, and vice versa.
Figure 6.12. Parts of the Hanau H2-158 Articulator.

A. Upper member
B. Lower member
C. Mounting plate
D. Mounting plate lockscrew
E. Condylar shaft
F. Post
G. Horizontal condylar guidance
H. Horizontal condylar guidance lockscrew
I. Horizontal condylar indication
J. Condylar element
K. Centric stop
L. Centric lock
M. Lateral condylar guidance and scale
N. Incisal guide pin
O. Incisal guide pin lockscrew
P. Incisal guide table
Q. Incisal guide table lockscrew
R. Cast support
S. Extension pin
6.9.12. Incisal (Anterior) Guide Pin and Lockscrew (N and O)
The incisal guide pin is a means of controlling the occlusal vertical dimension after the casts are mounted. The occlusal vertical dimension can be held constant or changed if needed.
6.9.13. Incisal (Anterior) Guide Table and Lockscrew (P and Q)
The incisal guide table helps preserve existing horizontal and vertical overlaps between upper and lower anterior teeth. This table can help develop proper horizontal and vertical overlaps when these tooth relationship factors are inadequate or absent.
6.9.14. Cast Support (R)
The cast support helps stabilize the maxillary cast as it is being mounted to the upper member of the articulator.
6.9.15. Extension Pin (S)
The extension pin provides support to the upper member when the upper member is opened 180 degrees.
¶ 6.10. Whip-Mix Articulator
The parts of this articulator are listed below (and in Figure 6.13):
6.10.1. Upper Frame (A)
The upper frame is the articulator equivalent of the upper jaw.
Figure 6.13. Parts of the Whip-Mix Articulator.

A. Upper frame
B. Lower frame
C. Mounting plates
D. Mounting plate lockscrew
E. Upright
F. Condylar element
G. Horizontal condylar guide
H. Horizontal condylar indication scale
I. Condylar guide clamp
J. Intercondylar distance spacer
K. Sideshift guide
L. Sideshift guide lockscrew
M. Incisal guide pin
N. Incisal guide pin lockscrew
O. Incisal block or guide table
P. Incisal guide table lockscrew
Q. Latch assembly
R. Facebow mounting pin
6.10.2. Lower Frame (B)
The lower frame is the articulator equivalent of the lower jaw.
6.10.3. Mounting Plates and Lockscrew (C and D)
The mounting plates are used for fixation of the patient’s casts to the upper and lower frames of the articulator. Like Hanau mounting plates, Whip-Mix plates are keyed and can be removed and accurately replaced.
6.10.4. Upright (E)
The upright is the articulator equivalent of a ramus of the mandible.
6.10.5. Condyle Element (F)
The condyle element is the articulator equivalent of the condyle of
the mandible. Whip-Mix condyle elements can be adjusted to three interelement (intercondylar) distances; small (88 mm), medium (100 mm), and large (112 mm).
6.10.6. Horizontal Condylar Guide and Condylar Indication Scale (G and H)
The condylar guide is the articulator equivalent of the patient’s glenoid fossa and articular eminence. The scale shows the angle at which the condylar guide is inclined to the horizontal plane.
6.10.7. Condylar Guide Clamp and Lockscrew (I)
One of the functions of the clamp and lockscrew is to maintain the condylar guide at selected inclinations.
6.10.8. Intercondylar Distance Spacers (J)
6.10.8.1. When the condyle elements are adjusted to small, medium, or large settings, the condylar guides have to travel in or out with them. The alignment of the condylar guides over the condyle elements has to be very precise, and the intercondylar distance spacers are responsible for the alignment. The spacers are placed on the shaft that holds the condylar guide suspended from the condylar guide clamp. Although no spacer is placed on the shaft for the small condyle element setting, one is used per side for the medium condyle element position and two are used per side for the large setting.
6.10.8.2. Because the intercondylar spacers are specific for the Whip-Mix articulator they are packaged for, they should not be interchanged or used with another Whip-Mix articulator. When not in use, the spacers should be placed on the incisal guide pin to ensure they remain with that articulator.
6.10.9. Lateral Condylar (or Sideshift) Guide and Lockscrew (K and L)
The sideshift guide and scale are the articulator’s sideshift controls. A standard Whip-Mix articulator (Model 8500) comes equipped with sideshift guides that only allow adjustable progressive sideshift. Another Whip-Mix model, the 2000 series, comes with curvilinear eminentia, a 7 1/2 degree progressive sideshift, and adjustable immediate sideshift guides.
6.10.10. Incisal (Anterior) Guide Pin and Lockscrew (M and N)
The incisal guide pin is a means of controlling the occlusal vertical dimension once casts are mounted. The occlusal vertical dimension can be held constant or changed if needed.
6.10.11. Incisal (Anterior) Guide Table and Lockscrew (O and P)
The incisal guide table helps preserve existing horizontal and vertical overlaps between upper and lower anterior teeth. The incisal guide table can also help develop proper horizontal and vertical overlaps when these tooth relationship factors are inadequate or absent.
6.10.12. Latch Assembly (Q)
The latch assembly is a device that centers the upper member over the condyle elements in a centric position when immediate sideshift guides are used. With the centric latch engaged, the upper member is secured to the lower member.
6.10.13. Facebow Mounting Pin (R)
The earpieces of a facebow attach to the pins when mounting a maxillary cast using the direct facebow mounting technique.
¶ Section 6B — Transferring Patient Information That Controls Mandibular Movements to Semiadjustable Articulators
¶ 6.11. Vertical and Horizontal Orientation of the Maxilla to Both Temporomandibular Joints
Adequate simulation of the vertical and horizontal orientation of the maxilla depends on how the maxillary cast relates to the condylar elements of the articulator when the cast is mounted to the upper member. Three methods may be used to establish the orientation of the maxillary cast to the articulator. They are the average method, the arbitrary facebow transfer method, and the kinematic axis facebow transfer method. The average method is discussed in paragraph 6.12 and the arbitrary facebow transfer method is discussed in paragraph 6.13. (The kinematic axis facebow method resembles the arbitrary facebow method enough that it will not be discussed further.)
¶ 6.12. Average Method
6.12.1. Hanau H2-158.
6.12.1.1. To mount a cast with this method, first place a rubber band around the condylar posts and the anterior guide pin (Figure 6.14).
(Ensure the top of the guide pin is flush with the upper member.) Then position the band on the pin’s lower mark and make the band parallel to the articulator’s horizontal plane.
Figure 6.14. Average Mounting of a Maxillary Cast in a Hanau H2-158 Articulator.

6.12.1.2. Using compound, sticky wax, or glue, secure the maxillary and mandibular cast together in MI or with a centric relation record. Orient the occlusal plane of the maxillary cast, using clay or wax support to fall on the plane of the rubber band. (If the maxillary cast represents a complete denture case, make the plane of the maxillary occlusion rim conform to the plane of the rubber band.)
6.12.1.3. Next, center the maxillary cast under the mounting plate while aligning the cast midline behind the incisal guide pin. The cast can now be attached to the plate with dental
stone. Orienting the maxillary cast in this way results in the following: the maxillary plane of occlusion is parallel to the horizontal plane of the articulator, the occlusal plane is the average vertical distance away from the temporomandibular joints, and the midline between the two maxillary central incisors is the average horizontal distance away from the two temporomandibular joints.
6.12.2. Whip-Mix.
6.12.2.1. This articulator was never intended to be used as a fixed-guide instrument. It has no convenient reference marks for average mounting of an upper cast (anterior guide pin reference grooves).
6.12.2.2. However, to use the articulator in this way, measure 40 mm down the lower frame from the under surface of a condyle ball and engrave a discreet mark (Figure 6.15). Do this on the left and right lower frame uprights. Then place a rubber band around the two engraved marks and around the anterior guide pin.
Figure 6.15. Notched Whip-Mix Upright.

6.12.2.3. The front part of the rubber band can now be adjusted so the band is parallel to the horizontal plane of the articulator (Figure 6.16).
Once the rubber band is positioned, perform an average upper cast mounting as for the Hanau H2-158.
¶ 6.13. Arbitrary Facebow Transfer Method
6.13.1. Mounting an upper cast for the semiadjustable or fully adjustable modes is done with a facebow transfer. A facebow is a caliper-like instrument that relates an upper cast to the condyle elements of an articulator in the same way a patient’s upper jaw relates to the temporomandibular joints (Figure 6.17).
6.13.2. Mounting an upper cast in this way is much more accurate than using statistical averages (Figure 6.18).
One advantage is that small alterations can be made to the occlusal vertical dimension without remounting the case. Another advantage is that the lateral tooth contact relationships developed for a prosthesis in the articulator are more likely to show up in the same way when the patient moves the lower jaw laterally.
Figure 6.16. Arbitrary (Average) Orientation of a Maxillary Cast to the Condyle Elements of a Whip-Mix.

Figure 6.17. Facebow.

6.13.3. Facebow shapes and mechanics differ slightly from brand to brand. Follow directions in the manufacturer’s instructions.
6.13.4. The use of a Hanau H2-158 facebow for mounting an edentulous upper cast in complete denture construction is described in Chapter 7, paragraph 7.47.2.
6.13.5. The use of a Whip-Mix facebow (earbow) for mounting a dentulous upper cast in fixed partial denture construction is described in Chapter 1, Volume 2.
Figure 6.18. Facebow Transfer.

¶ 6.14. Centric Relation
6.14.1. Once the upper cast is mounted, the lower cast must be articulated against it. It is up to the dentist to decide whether maximum intercuspation is adequate for articulating the lower cast or whether the articulation must be done with some form of maxillomandibular relation record.
6.14.2. Every position the mandible can assume in relation to the maxilla has a horizontal and a vertical component. The horizontal component represents the anteroposterior and lateral position of the condyles in the glenoid fossae. The vertical component is the prevailing vertical dimension between the maxilla and mandible (that is, the occlusal vertical dimension or some other vertical distance between the jaws).
6.14.3. When enough natural teeth remain, the casts might be mounted in MI. The way the teeth fit together controls the horizontal position of the lower jaw in relation to the upper, and the natural teeth in contact produce an occlusal vertical dimension. When an acceptable MI is gone, the centric relation position is used to horizontally orient the lower jaw, and the occlusal vertical dimension must be estimated. This situation is typical of complete denture problems.
6.14.4. The dentist records centric relation and the occlusal vertical dimension with a maxillomandibular relationship record (for example, record bases and record rims). The technician uses this record to articulate the lower cast against the upper cast. The use of a maxillomandibular relationship record to orient edentulous casts is described in Chapter 7, paragraph 7.48. For an example of a MI mounting with casts from dentulous patients, see Chapter 8, paragraph 8.40.2.
6.14.5. A complete mouth rehabilitation case requiring multiple crowns or fixed partial dentures involves the same kind of problem. When the dentist is finished preparing the natural teeth, maximum intercuspation is gone. The dentist must supply a maxillomandibular relationship record to mount the mandibular cast. (See Chapter 1, Volume 2, of this manual.)
6.14.6. After the lower cast is articulated against the upper cast, be acutely aware that changing the anterior guide pin setting changes the patient’s occlusal vertical dimension. In cases where the casts have been mounted at the patient’s occlusal vertical dimension (MI or centric relation), the pin-flush rule helps eliminate the need for remembering where the anterior guide pin was set.
6.14.6.1. According to the pin-flush rule, the following conditions should be met when the mounting is completed: the casts are at the occlusal vertical dimension, the pin is flush with the top of the articulator’s upper member (Hanau) or set at the zero reference line (Whip-Mix), and the pin contacts the anterior guide table.
6.14.6.2. The pin-flush rule does not apply to mountings where a maxillomandibular relationship record holds natural or artificial teeth apart at a distance other than the desired occlusal vertical dimension. In these situations, the following steps are performed in order. Mount the upper cast. Open the anterior guide pin by the estimated thickness of the maxillomandibular relationship record. Mount the lower cast. When you finish, remove the maxillomandibular relationship record. Reset the pin at the estimated occlusal vertical dimension and record the pin setting on the base of the upper cast. This will be the patient’s actual occlusal vertical dimension.
¶ 6.15. Angles the Articular Eminences Form With the Occlusal Plane
The slant of an articular eminence relative to the occlusal plane is a major determinant of a mandibular movement. The angle may be the same, or it may differ from side to side. After the patient’s casts are mounted on an articulator, the horizontal condylar guidances should be inclined to match the patient’s eminence-to-occlusal plane angles. The average method is discussed in paragraph 6.16; the interocclusal record method is discussed in paragraph 6.17.
¶ 6.16. Average Method
6.16.1. The average setting of the horizontal condylar guidances on the Hanau and Whip-Mix articulators are the same. In the average method, the horizontal guidance is set at the + 30 degree mark when the occlusal plane or plane of a record rim is mounted parallel to the horizontal plane of the articulator (Figure 6.19). The rationale for this procedure is that for the average patient, the angle formed by the articular eminence and the occlusal plane equal + 30 degrees.
Figure 6.19. Average Setting of Horizontal Condylar Guidance.

6.16.2. The Hanau and Whip-Mix articulators are machined so a horizontal condylar guidance readout of 30 degrees means the guidance is forming a 30-degree angle with the articulator’s horizontal plane. This leads to the conclusion that if a horizontal condylar guidance readout of 30 degrees is supposed to represent a valid average, the occlusal plane or plane of the record rim must be mounted parallel to the horizontal plane of the articulator.
6.16.3. If the anterior portion of the occlusal plane or plane of the record rim has been made to deviate downward from parallel with the horizontal, the 30 degree horizontal condylar guidance setting must be increased by the amount of the deviation. For example, if the anterior portion of the occlusal plane or plane of the record rim deviates downward from horizontal by an estimated 10 degrees, the horizontal condylar guidance must be set to read 40 degrees for the guidance and the occlusal plane or plane of the record rim to intersect at the valid average of 30 degrees (Figure 6.20).
6.16.4. If the anterior portion of the occlusal plane or plane of the record rim deviates upward from parallel with the horizontal, a 30-degree horizontal condylar guidance setting must be reduced by the amount of the deviation.
Figure 6.20. Horizontal Condylar Guidance Compensation for an Occlusal Plane Not Horizontally Oriented.

¶ 6.17. Interocclusal Record Method
6.17.1. Hanau Articulators. Adjusting the horizontal condylar guidance settings to the patient’s actual eminence inclinations requires mounting the maxillary and mandibular casts with a centric relation record or some centric position chosen by the dentist. In addition, the dentist must obtain a protrusive interocclusal relationship record from the patient. The protrusive record will be used to set the horizontal condylar guidance angles. See Chapter 7, paragraph 7.50.2, for a detailed description of this procedure.
6.17.2. Whip-Mix Articulator.
6.17.2.1. A protrusive interocclusal relationship record can be used to set right and left horizontal condylar guidances on the Whip-Mix articulator. In this respect, the method differs from directions given for the Hanau H2-158. After the upper member and cast are seated in the protrusive record, the horizontal condylar guidances are adjusted to touch the tops of the condylar elements.
6.17.2.2. The Whip-Mix articulator is somewhat more versatile than the Hanau H2-158. It accepts almost all lateral interocclusal relationship records, while the Hanau H2-158 does not. Another advantage of the Whip-Mix is that the horizontal condylar guidance and lateral condylar guidances (progressive sideshift) on one side can both be set from a single lateral interocclusal relationship record. (Another lateral record is needed to set the other side.)
6.17.2.3. Chapter 1, Volume 2, of this manual contains a further explanation of using lateral interocclusal relationship records in the Whip-Mix technique. Lateral interocclusal relationship records are preferred over a protrusive interocclusal relationship record for setting the horizontal condylar guidances of a Whip-Mix articulator.
¶ 6.18. Temporomandibular Joint Characteristics Governing the Timing and Direction of Laterotrusion
The articulator counterpart of this patient factor is the lateral condylar guidance feature of the Hanau H2-158 and Whip-Mix articulators.
6.18.1. Average Method. The average setting for the lateral condylar guidance on both Hanau articulators and Whip-Mix articulators is 15 degrees.
6.18.2. Interocclusal Record Method.
6.18.2.1. Hanau Articulators. The progressive sideshift of some semiadjustable articulators (Whip-Mix) can be set from lateral interocclusal relationship records made on the patient. The problem with a Hanau articulator is that it does not accept all lateral records. To compensate for this apparent lack of versatility, the manufacturer suggests the angle of a person’s eminence, occlusal plane, and amount of progressive mandibular translation (sideshift) are related. (For example, the steeper the angle of the eminence, the greater the sideshift.) Hanau devised the following formula to express this supposed relationship: L = H/8 + 12. That is, the lateral condylar guidance setting (L) is equal to the angle of the horizontal condylar guidance (H) divided by 8, to which 12 is added.
6.18.2.2. Whip-Mix Articulator. The dentist provides a right and left lateral record to set the corresponding horizontal condylar and lateral condylar guidances. (See Chapter 1, Volume 2, of this manual.) A standard Whip-Mix articulator comes equipped with sideshift guides, allowing only progressive sideshift. Four additional sets of guides can be bought, allowing 0.25, 0.50, 0.65, or 1 mm of immediate sideshift in conjunction with progressive sideshift. Using the theory that immediate sideshift increases as progressive sideshift increases, the Whip-Mix Corporation has made suggestions (shown in Table 6.1) for choosing among their range of sideshift guides.
Table 6.1. Suggestions for Choosing a Sideshift Guide.
| ITEM | A | B |
| Lateral Condylar Guidance Reading | Sideshift Guide | |
| 1 | 0 to 5 degrees | Standard guide (no immediate sideshift) |
| 2 | 5 to 15 degrees | 0.25 mm of immediate sideshift |
| 3 | 15 to 25 degrees | 0.50 mm of immediate sideshift |
| 4 | 25 to 35 degrees | 0.65 mm of immediate sideshift |
| 5 | over 35 degrees | 1 mm of immediate sideshift |
¶ 6.19. Distance (Space) Between a Patient’s Condyles (Intercondylar Distance)
6.19.1. Hanau Articulators. The Hanau articulators have a fixed intercondylar distance (110 mm). The word fixed means it cannot be changed. The 110 mm is supposed to represent the amount of space between an average person’s condyles.
6.19.2. Whip-Mix Articulator. The Whip-Mix 8500 series articulator has condyle elements that adjust to three interelement distances; small (88 mm), medium (100 mm), and large (112 mm). When the distance between the elements is changed, the condyle guidance mechanisms on the upper member must be aligned over the elements. The alignment is controlled by the intercondylar distance spacers. The 2000 and 3000 series have a fixed intercondyle distance of 110 mm.
6.19.2.1. Average Condyle Position. When the Whip-Mix articulator is used in the average position, the condyle elements are placed at the medium setting (one spacer in place).
6.19.2.2. Semiadjustable Mode. In the Whip-Mix system, a facebow transfer serves two purposes. It relates the upper cast to the condyle elements in the same way a patient’s upper jaw relates to the temporomandibular joints. In addition, it registers the approximate intercondylar distance. When a dentist uses a Whip-Mix facebow on a patient, the facebow indicates a small, medium, large, or intercondylar distance by an indicator on the front of the facebow. The condyle elements are adjusted to the proper setting before the upper cast is mounted.
¶ 6.20. Relative Presence or Absence of Anterior Guidance
Setting an articulator to accommodate this patient factor requires either maintaining existing horizontal and vertical overlaps between upper and lower teeth or developing new ones. The anterior guide table is the primary articulator control involved. In setting an anterior guide table, the following important considerations must be weighed:
6.20.1. When casts carrying natural teeth move in and out of MI, stone surfaces rub away. The anterior guide table can be set to help prevent this.
6.20.2. If the patient has sufficient natural teeth present, does the occlusion show group function or anterior guidance? Under ordinary circumstances, the patient’s natural guidance patterns should be maintained.
6.20.3. If natural teeth are badly worn or completely missing, will the occlusion be restored to show anterior guidance, group function, or bilateral balance? The dentist analyzes the restorative problem and sets the anterior guide table accordingly or directs the technician to set the proper anterior guidance.
6.20.4. After the table is set, the technician manipulates the horizontal and vertical overlap variables (anterior guidance or lack of it) on the prosthesis to conform to the occlusion scheme chosen. Until the technician develops a sense for the influence of the anterior guide table as a control, he or she should depend on the dentist for guidance.
6.20.5. A mechanical anterior guide table can be used with most articulators. The chisel edge of the anterior guide pin is used with the mechanical anterior guide table. This guide table can be used to prevent the abrasion of mounted stone casts and can provide guidance when setting denture teeth, but it cannot provide a permanent record of a patient’s anterior guidance.
6.20.5.1. To use the mechanical anterior guide table, mount the maxillary and mandibular casts appropriately onto the articulator. Carefully guide the maxillary cast into straight protrusive movement until the incisal edges of the maxillary incisors are brought into contact with the incisal edges of the mandibular incisors.
6.20.5.2. Rotate the anterior guide table to make contact with the chiseled surface of the anterior guide pin and tighten the locknut. Next, adjust the mechanical anterior guide table for right and left lateral movements.
6.20.5.3. Move the maxillary cast in a right lateral canine to canine guidance position. Elevate the anterior guide table’s lateral wing to contact the corner of the chiseled surface of the anterior guide pin and tighten the locknut to maintain the adjustment. Then adjust the left lateral wing in the same manner.
6.20.6. A custom anterior guide table can be made for Whip-Mix and Hanau Wide-Vue arcon articulators. The custom anterior guide table is made using the rounded end of the anterior guide pin. The table prevents the possible abrasion of the mounted stone casts during the manipulation of the articulator and can be used as a permanent record of the anterior guidance of the patient.
6.20.6.1. To fabricate a custom anterior guide table, mount the maxillary and mandibular casts appropriately onto the articulator. Lubricate the rounded end of the anterior guide pin with petroleum jelly.
6.20.6.2. Moisten the plastic anterior guide table with one or two drops of acrylic resin monomer. Mix autopolymerizing acrylic resin and place a 10 mm thickness of the acrylic resin on the anterior guide table. Once the acrylic resin reaches its doughy stage, close the articulator until the rounded end of the anterior guide pin penetrates the doughy acrylic resin and touches the anterior guide table.
6.20.6.3. Move the maxillary member of the articulator into a protrusive movement until the maxillary and mandibular anterior teeth meet end to end. Establish right and left lateral border movements to an end to end position of the teeth. Make all excursive movements while the acrylic resin is still doughy and contour any excess acrylic resin after polymerization is complete.
¶ 6.21. Proper Performance of a Lateral Excursion on an Articulator
6.21.1. When going to the trouble of developing specific lateral contacts between natural or artificial teeth in an articulator, it is reasonable to hope those contacts show up in the same way in the patient’s mouth. Reproducing the patient’s sideshift in an articulator is one of the most important factors in achieving this goal.
6.21.2. It is not enough to casually grasp the anterior guide pin of an articulator, pushing against it to move the upper member to the side, and call this a lateral excursion. The upper member of the articulator must be moved laterally in a very particular way to guarantee sideshift occurs in the amount corresponding to the lateral condylar guidance setting.
6.21.3. To move the Hanau H2-158 articulator, lock down the working side condyle against the centric stop and place a thumb on the working side condylar guide. To get full sideshift value, move the upper member toward the balancing side and push the condylar guide in the same direction (Figure 6.21). If the movement is done correctly, the shoulder of the condylar shaft will remain in contact with the external surface of the balancing condylar element during the entire course of the upper member’s lateral travel. Also, a space will develop between the condylar element and the brass stop external to the element on the working side. The space represents the full amount of sideshift the lateral condylar guidance setting allows (Figure 6.22).
6.21.4. To produce a proper lateral movement in a Whip-Mix articulator, place your thumb on the working side horizontal condylar guide and push the back end of the upper member toward the balancing side. Simultaneously, move the front part of the upper member in the same direction with your other hand. The objective is to keep the balancing side condyle element in contact with its sideshift plate during the entire lateral excursion (Figure 6.23). The sideshift is the amount of space between the working side condyle element and the sideshift plate.
¶ 6.22. Hanau Wide-Vue Series of Articulators
6.22.1. The Hanau Wide-Vue series of arcon articulators consists of eight basic models. The Wide-Vue models 183-1 through 183-4 have a closed condylar track, and the maxillary and mandibular members cannot be separated. The Wide-Vue II models 184-1 through 184-4 have an open condylar track, and the maxillary and mandibular members can be separated.
6.22.2. The lingual visibility with this series of articulators is excellent. The posterior openness allows tooth positioning and alignment with a minimum of visual obstruction from the body of the articulator. This type of articulator has a dual-end anterior guide pin which allows the use of a mechanical guide table and the fabrication of a custom guide table.
Figure 6.21. Manipulation of the Hanau H2-158 Articulator To Obtain Full Sideshift Value in a Lateral Movement.

Figure 6.22. Lateral Movement Incorporating Sideshift in the Hanau H2-158 Articulator.

¶ 6.23. Whip-Mix 2000-Series of Arcon Articulators
6.23.1. The Whip-Mix 2000-series of articulators consists of four different models; 2200, DB2000, 2240, and 2340.
6.23.2. The 2000-series of articulators have a redesigned frame which allows more space for mounting casts and improved posterior visibility. Also, a curved condylar guide and immediate sideshift have been incorporated into this instrument.
6.23.3. A new centric latch that allows a quick and stable return to the MI position, and a permanent 110 mm intercondylar width has improved the sturdiness of this instrument. Bilateral elastics have been incorporated to hold the maxillary and mandibular members securely together during excursive movements.
6.23.4. A unique and potentially useful innovation is the Accumount mounting system used in the manufacture of Models 2240 and 2340 articulators. During the production of these articulators, a special mounting plate has been attached to the lower frame, using a special fixture and low-fusing alloy.
6.23.5. The relationship between maxillary and mandibular mounting plates has been checked and standardized. The manufacturer states that, because of this unique mounting system, there can be an accurate interchange of mounted casts between two Model 2240 or 2340 articulators. This feature allows the casts mounted on one Model 2240 to be removed from the articulator and transported to a dental laboratory. At the laboratory, the casts are mounted on a second Model 2240 to have the prosthesis fabricated. The dental office and laboratory now require fewer articulators. Also, wear and tear on these sensitive instruments is reduced because they are not being sent through the mail.
6.23.6. Communication between the dentist and the dental laboratory now becomes even more critical. The dentist must provide all the necessary information for programming the articulator if the articulator is to be used effectively in reproducing mandibular movements.
Figure 6.23. Lateral Movement Incorporating Sideshift on the Whip-Mix Articulator.

DentalTechnology.org is dedicated to preserving, teaching, and advancing the craft of dental technology.
This resource is made possible by Russellville Dental Lab, a full-service dental laboratory in Russellville, Kentucky, serving clinicians across the USA for more than 70 years.